
The coronavirus outbreak is first and foremost a human tragedy, affecting hundreds of thousands of people. It is also having a growing impact on the global economy. This article is intended to provide business leaders with a perspective on the evolving situation and implications for their companies. The outbreak is moving quickly, and some of the perspectives in this article may fall rapidly out of date. This article reflects our perspective as of April 13, 2020. We will update it regularly as the outbreak evolves.
Mckinsey’s latest perspectives on the coronavirus pandemic.
In this note, we offer some of our latest insights on the COVID-19 pandemic, starting with a survey of the current epidemiology and the five dynamics leaders need to watch: the efficacy of the surge in critical care, the expansion of testing and other traditional approaches, the development of antibody testing, the unknown nature of immunity, and a wave of innovation that might produce treatments and vaccines.
We then highlight four of our many recently published articles, each designed to help senior executives lead through the crisis. In “How to restart national economies during the coronavirus crisis,” we offer a new framework to help business, economic, and public-health leaders around the world know when it would be safe to reopen portions of their domestic economies. “Europe needs to prepare now to get back to work—safely” provides Europe-specific insights on the same critical topic. Many Asian economies have already reopened in part. Drilling down even further, in “Winning the (local) COVID-19 war,” our colleagues explain how local leaders can take up the fight. And in “Could the next normal emerge from Asia?,” we consider the new behavior and ways of working, now being tested in Asia, that might soon become global standards.
These and many more articles are available in our collection of coronavirus thinking.
The outbreak is moving quickly, and some perspectives here may soon be out of date. This article reflects our perspective as of April 13, 2020. We will update it regularly as the crisis evolves.
COVID-19: Where we are, and where we might be heading
COVID-19 continues to spread rapidly around the world. Almost every country has reported cases, but the burden is asymmetrically distributed. In the past seven days (April 6–12), 46 percent of new confirmed cases have been reported in Europe and 39 percent in the United States. To an extent, that’s because countries are at different stages of the pandemic. Some that were effective at initial containment, such as Singapore and Hong Kong, have seen resurgence and are implementing additional measures to address it. Others, such as many countries in Western Europe, have seen the number of new cases plateau or begin to decline and are debating the right approach to reopening their economies. Some countries appear to be at the peak of infection and are urgently building surge capacity in their health systems. In other parts of the world, the number of cases is rising rapidly. Countries such as Russia and Turkey are seeing a recent acceleration. India too has experienced a significant increase in the number of cases since the beginning of April and has evolved its response strategy, including extending the nationwide lockdown.
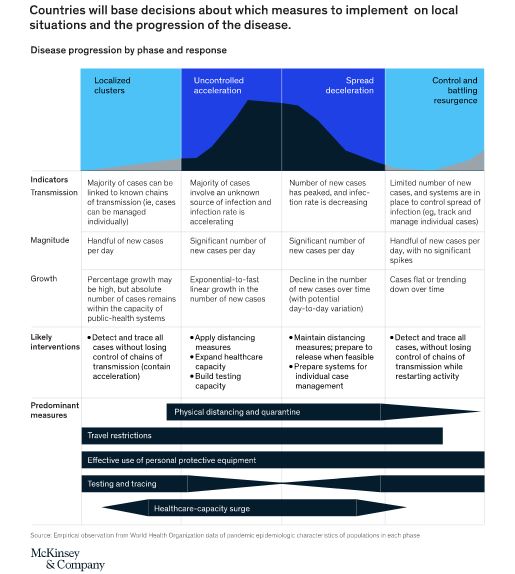
The public-health tools and approaches to be deployed vary considerably based on this status (Exhibit 1). Measures including physical distancing, travel restrictions, effective use of personal protective equipment (PPE), testing and tracing, and healthcare surge capacity require more or less emphasis, depending on epidemic phase and local context. Local use of these measures varies considerably—physical distancing may be near-impossible in crowded urban settings, for example, and the apps and digital tools for contact tracing like those used in China may not be acceptable in other parts of the world. Another challenge is the dependencies among these measures: to take one example, the timeliness and stringency of physical distancing measures substantially influences how other tools should be deployed.
Although a consensus has emerged around the use of physical distancing to slow transmission in many high-prevalence settings, a few countries, such as Sweden, are pursuing an alternative “herd immunity” strategy focused on protecting the most vulnerable populations while using only limited distancing measures to flatten the curve for others. The goals are to maintain many aspects of economic and social life today and, over time, to develop a large enough pool of exposed people (about 70 to 80 percent) to “protect the herd.” Other countries are closely watching the outcome of this approach.
The months ahead will probably be quite volatile and dynamic. It now appears likely that some places will experience a local resurgence asrestrictions are lifted and economies reopen. That will influence countries at the earliest stages. For example, Singapore has seen a resurgence mainly from imported cases, which have led to local transmission; this suggests that restrictions on international travel may continue. As China gradually reopens, the tactics it used (including group-based isolation models and setting a norm of wearing masks in the workplace) and their efficacy will inform approaches around the world. Western Europe’s experience in relaxing restrictions, and the most successful approaches there, will inform the approaches deployed in the United States.
Considering the variety of approaches in use, public understanding and consensus will evolve day by day. We will continue to find out more about the coronavirus—how it is mutating, the duration of immunity, its transmission dynamics, and so on. For example, it now appears that the virus probably won’t be highly seasonal, given the recent rapid growth in a number of hot spots in the Southern Hemisphere. But it is still possible that the arrival of summer in the Northern Hemisphere will slow transmission somewhat, as some studies in both labs and natural contexts suggest.
With all this in mind, we believe that leaders should closely watch five health-response dynamics in the coming weeks:
The efficacy of the health-system surge and how it is maintained over time. Countries with rapidly increasing numbers of cases are finding ways to expand their critical-care capacity massively. Their ability to do so, and to push mortality from COVID-19 to lower levels, will not only save lives but also engender confidence in their health systems’ ability to manage a resurgence. Over time, as cases plateau and then decline, there will be questions about how long to maintain surge capacity while also guarding against resurgence. Providers will be under pressure to consider the broader context of a capacity surge; for example, in the United States, the mass cancellation of elective medical procedures and the associated financial hardship for many providers is likely to force difficult discussions about which procedures should be allowed to restart, and when. Other effects of surge capacity, on vaccine-preventable diseases and maternal and child health, will also be critical to monitor.
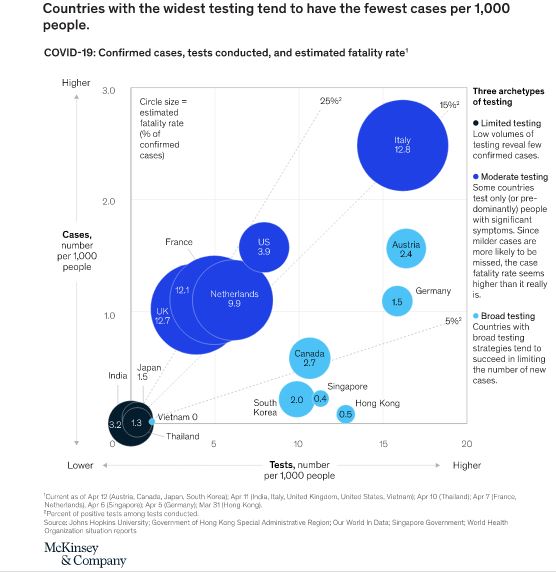
The scaling of traditional public-health approaches. In parallel with the surge in critical care, countries also need to think about building surge capacity in traditional public-health approaches—disease surveillance, contact tracing, and targeted quarantines. Such a surge must build on current efforts to scale viral testing rapidly, mostly through RT-PCR2 machines. Exhibit 2 shows the somewhat surprising relationship between testing and the number of cases—generally, countries that have tested more people have diagnosed fewer cases per thousand people. Moreover, to detect and control flare-ups quickly, widespread access to viral testing will become increasingly important as countries and cities prepare to relax distancing measures. In some countries, this testing capacity could be paired with at-scale contact tracing, with privacy-by-design embedded; and quarantine facilities to help localize hot spots and prevent a broader resurgence.
The development of antibody testing and understanding of sero-prevalence. We have little idea how many people have been exposed to this coronavirus. One recent study in a hard-hit area of Germany showed that about 14 percent of the population has been—far from the levels of exposure required for herd immunity to emerge but higher than many had expected.3 A lot of other studies are underway to assess the portion of the population exposed to COVID-19. If individual or herd immunity is to play a meaningful role in reopening, antibody tests to measure exposure must be widely available. While many such tests are being developed, their accuracy and availability have been challenged. The arrival of accurate, widely available antibody tests will help countries understand how close they are to achieving herd immunity and whether they can use immunity as a meaningful signal to start reopening.
The nature of immunity. People exposed to other coronaviruses have exhibited durable immunity for several years after exposure. Everyone hopes the same holds true for the novel coronavirus, but we don’t know for sure. Emerging reports of recovered patients testing positive again on RT-PCR acute-infection tests raise questions about reactivation, as do studies in China showing very low levels of antibodies among some infected people. While it is unlikely that the duration of immunity is short, any new information about this issue would require a significant shift in strategy.
Innovation. There has been an unprecedented burst of global pharmaceutical R&D related to COVID-19. Today, more than 130 therapeutic candidates and 80 vaccine candidates are under consideration across a range of modalities and use cases, such as treatment of severe disease and pre-exposure prophylaxis. If drugs already approved for other indications prove effective in treating COVID-19, they could be deployed most quickly, but in coming months readouts on experimental new drugs will also arrive. The massive scale-up of clinical trials—especially randomized placebo-controlled studies—will provide evidence to guide clinical decisions. Similarly, the unprecedented consortium of plasma companies generates hope that hyperimmune immunoglobulin can be developed quickly. Seven vaccines are already being tested in humans.4 Although at-scale production and distribution is not likely for 12 to 18 months after a successful trial, these vaccines would provide a critical element in the armamentarium against COVID-19. For all these innovations, a central challenge will be rapidly scaling up production to meet global needs.
Getting back to work: Four insights
The pandemic’s economic challenges are unprecedented. Since the crisis began, McKinsey has published more than 70 articles on the extraordinary public-health and economic impact, as well as the ideas that government and business leaders need to safeguard lives and livelihoods. In the past week, four articles have captured the attention of leaders around the world. We summarize these articles here and invite you to take in the full collection.
The threat of COVID-19 to lives and livelihoods will fully resolve only when enough people are immune to the disease to blunt transmission, either from a vaccine or direct exposure. Until then, governments that want to restart their economies must have public-health systems that are strong enough to detect and respond to cases.
The first and most obvious factor in determining readiness is the number of new cases in a given area. Regions with significant ongoing transmission should expect that restarting economic activity will only lead to more transmission. Case numbers and, more importantly, hospitalizations need to be low enough for a health system to manage individually rather than through mass measures. A second factor in thinking about this is the strength of the systems in place for detecting, managing, and preventing new cases, including adequate medical capacity, especially of intensive care units (ICUs), for those with severe disease; the ability to perform a diagnostic test for COVID-19 with a fast turnaround time; and several other elements.
If we combine a system’s level of strength with an assessment of the intensity of virus transmission, we can evaluate any region’s readiness to restart activity (Exhibit 3). These two dimensions determine four stages of readiness to reopen the economy, with Stage 4 the least ready and Stage 1 the most.
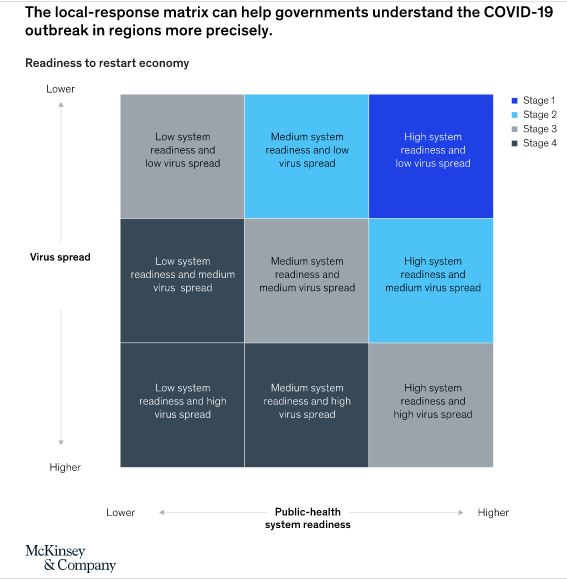
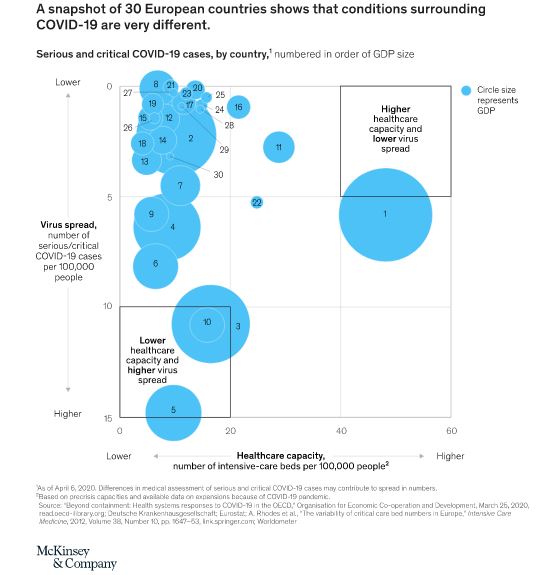
As European countries begin to consider how to exit lockdowns, local leaders are often the people best placed to evaluate conditions and impose measures that maximize economic recovery while protecting public health. Decisions about which measures to deploy, when and where, should be made locally—if possible, district by district—because there are material differences in the severity of the crisis and economic circumstances (Exhibit 4).
Authorities will need three essential elements to ensure robust implementation. First, leaders will require effective, ready-to-act local-authority structures. In Italy, regional governments collaborated with Rome to establish a national lockdown that allowed regions to apply more stringent rules as necessary.
Second, solutions and directives must be clear and simple, so that the public and businesses can understand them. This might require using new communication channels, such as mobile messaging.
Third, measures must be consistent. If the guidance one day is that shops can admit five people at a time for six hours a day and in the next week that rule changes to two people for eight hours, the results will be irritation, noncompliance, and the erosion of trust in public authorities.
Local US leaders, such as mayors and governors, have an outsized role in the fight against COVID-19. We see six domains for engagement:
Foundational public health. We assessed 23 public-health interventions and identified the most fundamental ones.
Societal compliance. We monitored different approaches to ensure compliance and found a steeper decline in infections where communities enforced policies tightly (through arrests, for example) than in those that used only fines.
Health-system capacity. To prevent demand for healthcare services from outstripping supply, we found that at least a doubling of critical-care capacity is probably possible and necessary, at least temporarily, across most parts of the United States.
Industry safeguards. If the risk of contagion continues for 12 to 18 months, public- and private-sector leaders should promote the most effective adaptations and safeguards to economic activity, including physical barriers, face guards, physical distancing, health screenings before entry, and generous and flexible sick leave. Sectors will vary in how critical they are and their ability to safeguard.
Protection of the vulnerable. COVID-19 is especially destabilizing for vulnerable populations, including people with chronic physical- or behavioral-health conditions, limited mobility, advanced age, and unmet health-related social needs, such as food and housing insecurity. Each will require targeted interventions.
Economic health. Local leaders need to develop a fact base on their economies and then ensure that money from new and current programs gets into the hands of citizens quickly and easily.
‘Could the next normal emerge from Asia?’
by Oliver Tonby and Jonathan Woetzel
The COVID-19 outbreak began in Asia—but so have early indications of containment, new protocols, and the resumption of economic activity. Although the risk of another outbreak remains, economic-activity indicators in China suggest that urban activities are returning to pre-outbreak levels. Traffic congestion and residential-property sales are close to where they stood in early January 2020. Air pollution and coal consumption have returned to 74 and 85 percent, respectively, of their January 1 levels. A recent McKinsey survey of 2,500 Chinese consumers indicates “cautious optimism”—a gradual regaining of confidence, which should increase spending. At this moment, strong public-health responses in China, Singapore, and South Korea appear to have been successful. Significant evidence indicates that the curve of cumulative confirmed COVID-19 patients in Asia is becoming flatter.
As companies in the region resume activity, they may be the world’s first to shape the “next normal.” What will that look like? Four dimensions could define it:
Rethinking social contracts. In crises, the state plays an essential and expanded role, protecting people and organizing the response. This power shift transforms long-held expectations about the roles of individuals and institutions.
Defining the future of work and consumption. The crisis has propelled new technology across all aspects of Asian life, from e-commerce to remote-working and -learning tools, including Alibaba’s DingTalk, WeChat Work, and Tencent Meeting. New working and shopping practices will probably become a permanent fixture of the next normal.
Mobilizing resources at speed and scale. Within weeks, China added tens of thousands of doctors and hospital beds. Several governments invested in new tools to map transmission and rolled out huge economic-stimulus plans. Asia has a proven ability to mobilize resources in a crisis.
Moving from globalization to regionalization. The pandemic has exposed the world’s risky dependence on vulnerable nodes in global supply chains. China, for example, accounts for about 50 to 70 percent of global demand for copper, iron ore, metallurgical coal, and nickel. We could see a massive restructuring as production and sourcing move closer to end users and companies localize or regionalize their supply chains.
About the authors
Matt Craven, MD, is a partner in McKinsey’s Silicon Valley office. Shubham Singhal is a senior partner in the Detroit office. Matt Wilson is a senior partner in the New York office.











